Castleman Disease
74 year-old-man

|
|
TP |
Alb |
α1-gl |
α2-gl |
β-gl |
γ-gl |
IgG |
IgA |
IgM |
IgE |
|
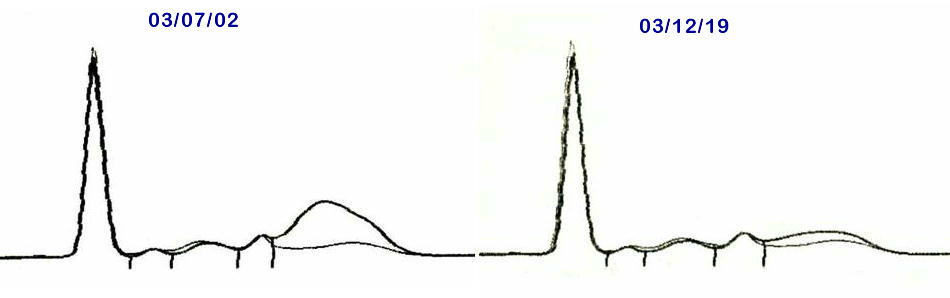
03/07/02 |
8.5 |
3.14 |
0.20 |
0.54 |
0.44 |
4.18 |
4380 |
453 |
42 |
4897(IU) |
|
03/12/19 |
6.7 |
3.66 |
0.16 |
0.51 |
0.58 |
1.78 |
NA |
NA |
NA |
NA |
(g/dL mg/dL)
CLINICAL COURSE:
This 72-year-old man was initially diagnosed as having systemic lupus erythematosus (SLE), because he had had febricula, polyarthralgia and rapid weight loss, with the following abnormalities in laboratotory examinations; hypergammaglobulinemia, slightly elevated anti-DNA antibody titer /23 U/mL (normal; ≦6 U/mL), thrombocytopenia/6.2×10^4/μL, and elevated serum creatinine/1.52 mg/dL. His urinalysis showed a slightly positive proteinuria (±). Serum C-reactive protein (CRP) was 1.3 mg/dL and C3, C4 were 24.3, and <1.4 mg/dL, respectively.
The histopathology of renal biopsy showed marked interstitial plasma cell infiltration, without any glomerular involvement. Neck lymph nod biopsy specimens showed marked inter-follicular plasma cell infiltration. The morphology of the infiltrating plasma cells was almost normal, with also normal κ/λ ratio.
These histopathologic feature was compatible with that of Castleman disease (plasma cell type). Corticosteroid therapy with 10 mg/d of prednisolone was done, and his subjective symptoms and the hypergammaglobulinemia and elevated anti-DNA antibodies were recovered five months later (Figures and Table).
COMMENTS:
Castleman disease (CD) is a essentially benign lymphoproliferative disorder which develops weight loss, fatigue, lymph nod swelling, etc. as clinical symptoms. This disease is divided into a hyaline vascular and plasma cell histopathologic patterns, with intermediate variants (1). The former is much more frequent (90% of the disease) and usually involves localized lymph nods. The latter (10%) develops multicentric lesions and often shows systemic symptoms including autoimmune phenomena such as lupus like disease (2).
Although the cause(s) of this lymphoploriferative condition is unknown, some contributing factors such as Epstein Varr virus infection, or implication of IL-6 due to various causes are considered as the etiology.
The marked hypergammaglobulinemia which is sensitive to small dose corticosteroid is a characteristic property of CD, in contrast to that of SLE, in which high dose corticosteroid is necessary to reduce the elevated gammaglobulin level. This suggests that CD is a disorder arisen only from B-cell system, whereas SLE is more complicated disease, in which systemic immune mechanisms and immunocytes, including not only B-cell but also T-cell system, are widely involved.
REFERENCES:
1. Palestro G, Turrini F, Pagano M, Chiusa L. Castleman's disease. Adv Clin Path 1999: 1-2:11-22.
2. Kojima M, Nakamura S, Itoh H, et al. Systemic lupus erythematosus (SLE) lymphadenopathy presenting with histopathologic features of Castleman's disease: a clinicopathologic study of five cases. Pathol Res Pract 1997;193:567-71.
ACKNOWLEDGEMENT:
The presented case was furnished by Division of Rheumatology and Collagen Disease of Osaka City University Hospital. I thank Drs. Naoki Sugimoto, Nobuo Negoro and their colleagues for their permission to make this presentation. (T.Inoue, Oct. 19, '07)