Recurred Liver Cirrhosis after Embolization (TAE) for
Hepatocellular Carcinoma
|
Date |
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma (g/dL) |
|
7/20 |
7.2 |
3.5 |
0.28 |
0.60 |
0.78 |
2.0 |
|
9/20 |
8.0* |
4.0* |
0.18 |
0.30 |
(beta + gamma →) |
3.5 |
*:Data of soon after supplemental administration of albumin
CASE: 69-year-old woman
DISEASE: Hepatocellular carcinoma (HCC)
COMMENTS:
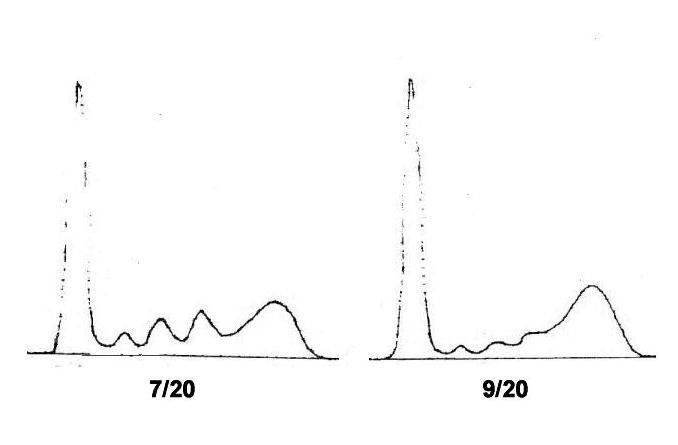
The solitary HCC of this patient was developed after the long-term historry of chronic hepatitis followed by liver cirrhosis due to HBV infection. Just before the start of the arterial embolization (July/20), her AST and ALT were 105 IU and 55 IU, respectively, and the choline esterase was 0.33 delta-pH. The electrophoretic pattern showed an elevated gamma globulin level, however the changes in other globulin fractions were not so conspicuous, and the pattern seemed, if anything, to be compatible with that of chronic hepatitis and not of cirrhosis (Figure 7/20).
At Aug.8 and Aug.30, arterial therapies of transarterial chemoembolization (TAE) for the solitary tumor were done twice with sponzel and mitomycin C (5 mg).
After the treatment, the patient was led into a severe hepatic failure. and the electrophoretic pattern dramatically changed to the patten of typical liver cirrhosis characterized by significant hypergammaglobulinemia, and decreased levels in alpha-1, alpha-2 globulins and especially in beta globulin (Figure 9/20). These clinical and serological changes indicated that the patient's HCC cells, by which her small reserve of the liver function must had been supported, were almost completely eliminated by the TAE. In other words, the successful eradication of tumor cells ironically resulted in the recurrence of her original hepatic failure.
If the hepatic function reserve were not precisely evaluated, the therapeutic eradication of HCC cells might be a risky option.
REFERENCES:
1. Barnett CC, Curley SA. Ablative techniq1ues for hepatocellular carcinoma. Semin Oncol 1001;28:487-96.
2. Gunji T, et al. Long-term outcomes of transcatheter arterial chemoebolization with autologous blood clot for unresectable hepatocellular carcinoma. Int J Oncol 2002;21:427-32.
3. Mulcahy MF. Management of hepatocellular carcinoma. Curr Treat Options Oncol 2005;6:423-35.
T.Inoue (Jan.2007)