M-protein and ZTT
INTRODUCTION
In European countries and United States, zinc sulfate turbidity test (ZTT), a simple colloid turbidity reaction, is now considered to be of no use as a clinical screening test. because of its "poor specificity". However, I consider that "poor specific" is, in other words, "wide ranged", and ZTT just has ability to detect disproteinemias caused by various disorders.
In this study, I am going to show the association of ZTT with monoclonal gammopathies, in which not only the class but also subclass of immunoglobulins could be recognized by ZTT.
ZTT and HYPERGAMMAGLOBULINEMIA
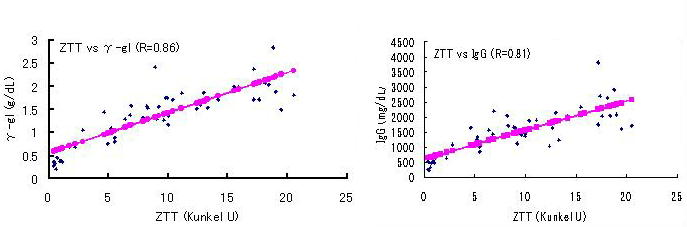
As an assumption, I tried to confirm the correlation coefficient of ZTT (Kunkel Unit) with serum IgG concentration (g/dL). The data were collected from 52 subjects with various clinical conditions, including normal subjects, collagen diseases, chronic liver diseases, and nephrosis, etc. while M-proteinemia was excluded.
The following numerical formula was obtained from these samples.
ZTT (KU) = 7 ×IgG (g/dL)-1 (r = 0.81, P<0.001)
Based on the result, I would like to propose a more simple and practical rough formula;
ZTT / 8 = IgG (or gamma globulin)(g/dL)
CASE PRESENTATIONS
Monoclonal gammopathy is not so uncommon in elderly population, especially so called a "benign" clinical state, monoclonal gammopathy of undefined significance (MGUS)、 is occured in up to 2 percent of persons 50 years of age or older (1). Thus, three clinical conditions are included in monoclonal gammopathy; overt, and smoldering myelomas (MM and SMM), and MGUS. The diagnostic criterion of these conditions proposed by Southwest Oncology Group (SWOG). is shown in the table.
Table: The diagnostic criterion of M-proteinemia by Southwest Oncology Group (SWOG)
|
|
plasma cell population in bone marrow (%) |
IgG M-protein (g/dL) |
IgA M-protein (g/dL) |
|
MM |
> 30 |
> 3.5 |
> 2.0 |
|
SMM |
10 〜 30 |
3.0 〜 3.5 |
≦ 2.0 |
|
MGUS |
≦ 10 |
≦3.5 (or ≦ 3.0) |
≦ 2.0 |
The presented cases 1, 2, and 3 were diagnosed as having MM, SMM and MGUS, respectively according to the SWONG criterion. The values of ZTT of these three patients were commonly elevated regardless of their clinical stage and type of light chain.
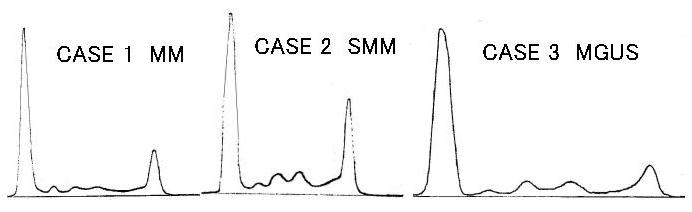
CASE 1: Overt IgG MM. 61-year-old woman. Punched out lesions were present. (λ)
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
ZTT |
TTT |
|
4.7 |
2.9 |
0.18 |
0.27 |
0.36 |
1.0 |
1288 |
49 |
44 |
> 20 |
> 8.0 |
CASE 2: IgGSMM. 56-year-old man. The plasma cell population of at this stage (1979) was 5 percent with atypical cells. He died of renal failure due to overt MM at 1993. (κ) The immunoelectrophoretic (IE) patterns are shown below.
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
ZTT |
TTT |
|
8.2 |
4.2 |
0.25 |
0.66 |
0.74 |
2.3 |
2743 |
86 |
95 |
> 20 |
> 8.0 |

CASE 3: IgG MGUS. 58-year-old man. The plasma cell pupulation is 1 percent in his bone marrow.
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
ZTT |
TTT |
|
8.3 |
4.3 |
0.15 |
0.47 |
0.53 |
0.87 |
1580 |
53 |
45 |
11.3 |
1.8 |
In contrast, the ZTT levels of two cases with overt MM shown as case 4, and 5, whose M-bows were located in the fast gamma position, were disproportionately low to their IgG levels.
From these findings, it is assumed that there must be two types of IgG including groups of the reactivity to zinc ion is maintained (= ZTT positive) and lost (= ZTT negative).
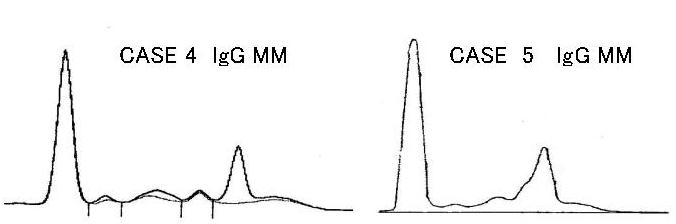
CASE 4: IgG MM. 64-year-old woman. Her IE pattern is shown below.
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
ZTT |
TTT |
|
7.5 |
4.5 |
0.17 |
0.43 |
0.62 |
1.83 |
2478 |
224 |
159 |
2.4 |
0.8 |
CASE 5: IgG MM. 50-year-old man.
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
ZTT |
TTT |
|
8.3 |
4.3 |
0.15 |
0.47 |
0.53 |
0.87 |
2993 |
63 |
117 |
0.9 |
1.2 |
The electrophoretic position of four IgG subclasses were shown in the figure (2). There is only IgG1 in the cathodic end of IgG, meanwhile the IgG4 or IgG2 may be the component of anodic end of IgG.
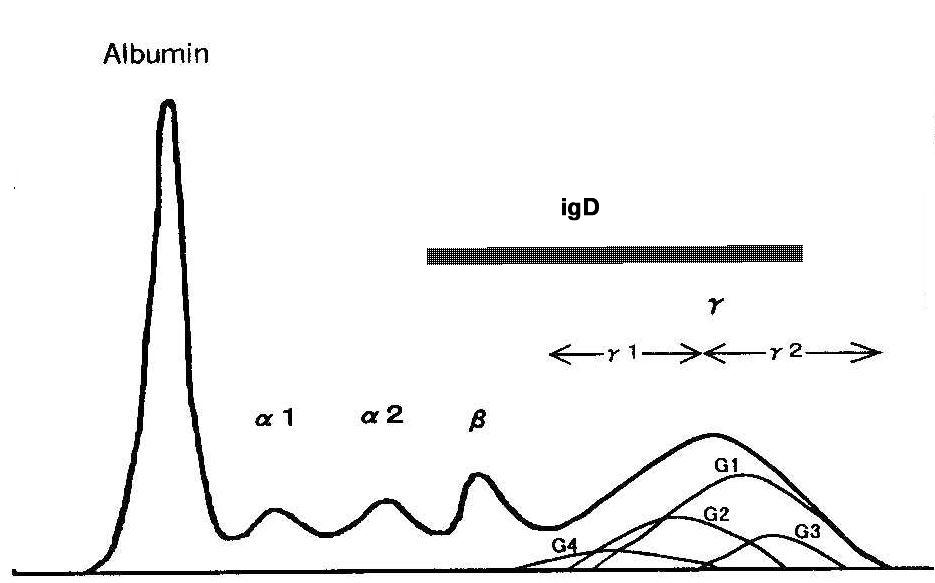
Then, it must be reasonable to understand that the M-proteins of presented cases 1, 2, and 3 belong to IgG1, and the M-bows of case 4, and 5 are IgG4 (or IgG2).
As seen in these observations, it is very interesting that zinc ion may react with only IgG1 (or possibly IgG3) molecules but not with IgG4 (or IgG2). The following mechanismus is now accepted as the process of ZTT; colloidal solution may become unstable and the precipitation may occur when Zn++ ion react with imidazole radicals which are the ubiquitous component of somatic proteins. According to this explanation, imidazole radicals must be rich in IgG1 but not in IgG4 or IgG2.
The reasons where are the difference in molecular construction and in reactivity to zinc sulfate ion between these IgG subclasses are unknown and must be clarified, and the immunochemical analysis also is needed to discriminate the difference in reactivity of IgG subclasses to zinc sulfate ion (3).
Case 6 is the serum electrophoretic pattern of IgM myeloma (Waldenstroem's macroglobulinemia). The ZTT was elevated in spite of IgG was remained in normal level. In general, levels of ZTT are assumed to be influenced by the concentration of many serum proteins, especially of IgM. This patient's elevated ZTT may explained by this assumption.
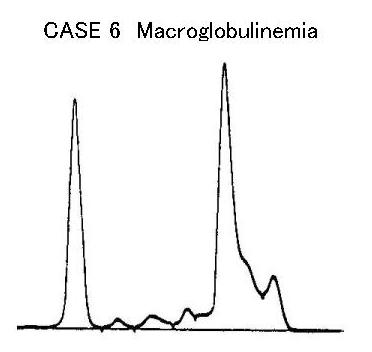
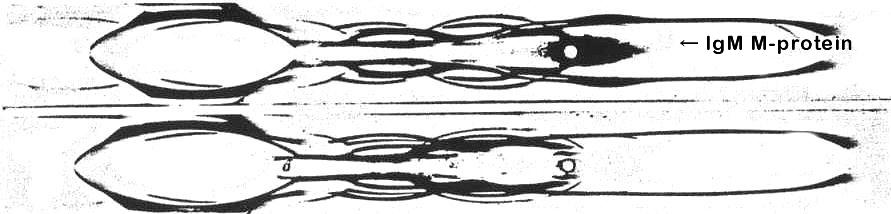
CASE 6: Waldenstroem's macroglobulinemia. 50-year-old man. The IE pattern is shown below.
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
ZTT |
TTT |
|
10.7 |
3.2 |
0.16 |
0.33 |
0.31 |
6.7 |
1001 |
19 |
15855 |
> 20 |
> 8.0 |
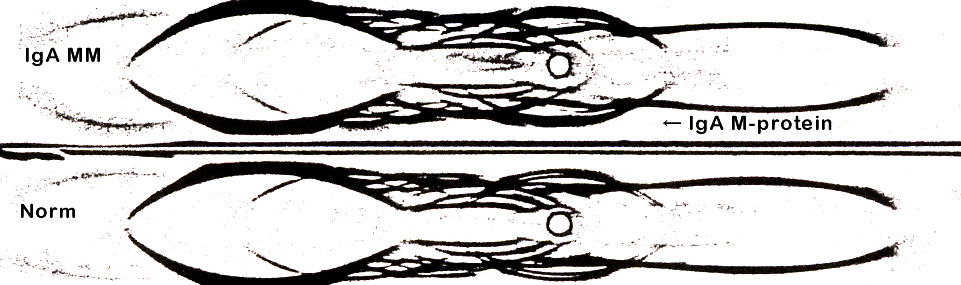
In IgA and IgD MM presented as cases 7 and 8, their ZTT were markedly decreased. The mechanism of the decrease is also unknown.
In clinical practice, it must be remember that the ill-matched low ZTT to serum gamma globulin level is occasionally the first clue to detect IgA, IgD and sometimes IgG MM.
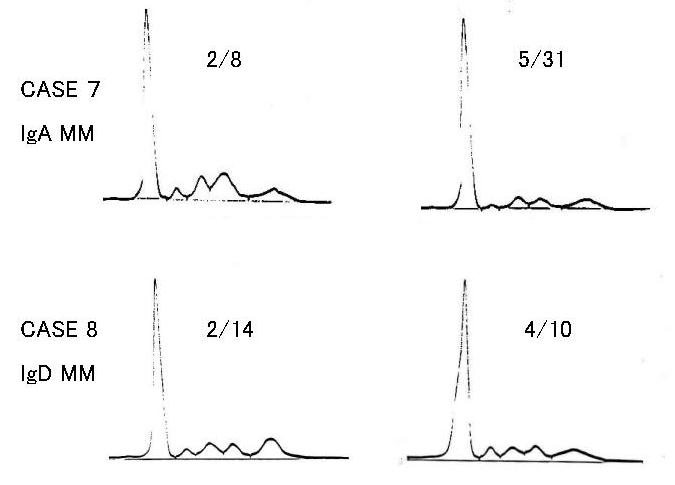
CASE 7: IgA MM. 59-year-old man. The plasma cell population in his bone marrow was 20 percent. He was treated with melpharan and prednisolone. The IE pattern is shown below.
|
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
ZTT |
TTT |
|
2/8 |
6.9 |
3.8 |
0.28 |
0.70 |
1.3 |
0.78 |
732 |
1168 |
40 |
0.3 |
1.0 |
CASE 8: IgD MM. 60-year-old woman. He was initially diagnosed as having severe renal failure of 13.8 mg/dL of creatinine. He was once recovered by hemodialysis and the medication with melpharan and prednisolone. His IE pattern at 2/14 is shown below.
|
|
TP |
Alb |
alpha-1 |
alpha-2 |
beta |
gamma |
IgG |
IgA |
IgM |
IgD |
ZTT |
TTT |
|
2/14 |
5.2 |
3.3 |
0.18 |
0.48 |
0.41 |
0.82 |
424 |
44 |
2 |
630 |
0.2 |
1.3 |
|
4/16 |
5.0 |
3.6 |
0.23 |
0.33 |
0.37 |
0.52 |
650 |
48 |
1 |
60 |
NA |
NA |

CONCLUSION
ZTT is still a sensitive and reliable clinical screening test, and its value must be realized again.
(T.Inoue Nov.07)
REFERENCES
(1).Kyle RA, et al. A
long-term study of prognosis in monoclonal gammopathy of undetermined
significance. N Engl J Med 2002;346:546-9.
(2). Miyagawa N, et al. Studies on the
relationship between serum colloidal reactions (ZTT and TTT) and IgG
subclasses, especially IgG1 and IgG2. Microbiol Immunol 35;1991:59-66.
(3). Ohtake
H, et al. Q&A on electrophoresis. Progress in AES '98. 1998: pp104-23. Olympus
Co. Tokyo. (in Japanese)